











How does Osteopathy relieve pain?
 Patients often report immediate and significant pain relief following spinal and peripheral joint manipulation. As well as relieving mechanical irritation of the joint cartilage by decompressing articular surfaces these corrective techniques have been shown to cause stimulation of proprioceptive nerve endings (mechanoreceptors) in the spinal facet joint or peripheral joint capsule, and associated ligaments sending a barrage of sensory input centrally to the spinal cord resulting in reflex inhibition of pain transmission to the brain by closing the "Pain Gate" within the dorsal horn of the spinal cord. Blocking pain or closing the pain gate is central to pain management. One way the brain can do this is by producing its own painkillers. Studies have shown increases in beta-endorphin levels after spinal manipulation but not after control interventions. These painkillers meet the pain signals in the spinal cord and block them (or close the gate).
Patients often report immediate and significant pain relief following spinal and peripheral joint manipulation. As well as relieving mechanical irritation of the joint cartilage by decompressing articular surfaces these corrective techniques have been shown to cause stimulation of proprioceptive nerve endings (mechanoreceptors) in the spinal facet joint or peripheral joint capsule, and associated ligaments sending a barrage of sensory input centrally to the spinal cord resulting in reflex inhibition of pain transmission to the brain by closing the "Pain Gate" within the dorsal horn of the spinal cord. Blocking pain or closing the pain gate is central to pain management. One way the brain can do this is by producing its own painkillers. Studies have shown increases in beta-endorphin levels after spinal manipulation but not after control interventions. These painkillers meet the pain signals in the spinal cord and block them (or close the gate).
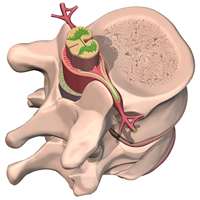
A second mechanism is that osteopathic spinal manipulation, by mechanically opening the intervertebral foramina (IVF), decreases pressure on the dorsal roots. Substantial evidence shows that the dorsal nerve roots and dorsal root ganglia are susceptible to the effects of mechanical compression. Compressive loads as low as 10 mg applied to dorsal roots increase the discharge of Group I, II, III & IV afferent (sensory) nerve endings. This compression can also alter non impulse-based mechanisms (eg, axoplasmic transport) and cause oedema and haemorrhage in the dorsal root. Spinal manipulation mechanically decreases the pressure in the IVF by gapping the facet joints and opening the IVF. For instance, the synovial space of the lumbar facet joints increases by about 0.7 mm in individuals receiving manipulation. This doesn't seem like much, but as with any therapy there is usually a course of care involved. Even in moderate stenosis patients treated by osteopaths typically see significant pain reduction following a period of 1-2 weeks of treatment.

City Clinic Of Osteopathic Medicine
T: 020 7796 0095
M: 07799 416 181
Consulting Rooms:
London – City
Smithfield EC1 & EC2, EC3, EC4
